
In plain sight: the skilled migration story hiding inside every diversity statistic
On what the workforce data shows when you read it from the other direction

My mother trained as a nurse at Chris Hani Baragwanath Hospital. It’s the largest hospital in Africa and eighth largest in the world (flex). She worked as a nurse from the late 80s into the 2000s. Having built her career in that environment, she’s incredibly sharp in crisis, has angelic patience and is entirely too practical for most conversations. In the early 2000s, several UK agencies were aggressively recruiting healthcare workers from Southern Africa to come and work in the NHS. Many of my mom’s peers took up the opportunity. She declined (I suspect) because she had married a Zulu man and, in his estimation, that wouldn’t be right for the family. Patriarchy: one. NHS staffing crisis: nil.
I have thought about that story a lot since starting this essay, because the recruitment of my mother was not an isolated acknowledgement of her excellence. It was a program defined by a systematic, government-adjacent effort to recruit African nurses into a healthcare system that cannot train enough of its own.
This emigration of highly skilled workers from one region to another is commonly referred to as a brain drain. I want to suggest that the name is doing considerable flattering work on behalf of the countries doing the recruiting, and that the more accurate word is extraction.
THE NUMBERS, WHICH ARE EMBARRASSING FOR EVERYONE
I’ll start with the NHS because it’s a fairly straightforward case to make. As of 2025, the General Medical Council reported that approximately 138,400 licensed doctors working in the UK qualified abroad, constituting 42% of the total medical workforce. They note themselves as one of the most diverse employers in the world. One in five NHS staff overall report a non-British nationality, a proportion that climbs to 36% among doctors and 30% among nurses. In 2025 the most common non-EU nationalities in the NHS were Indian, Filipino, and Nigerian. Nigeria is a country with a doctor-to-patient ratio of approximately 1 to 9,000 people, against the WHO recommended minimum of 1 to 600. So, Nigeria is simultaneously one of the largest suppliers of doctors to the NHS and has one of the most significant shortages in the world. Hmm, why do we think that is?
Let me show you what this looks like when you put it in a table, because numbers have a way of saying things politely that I can only say less politely.
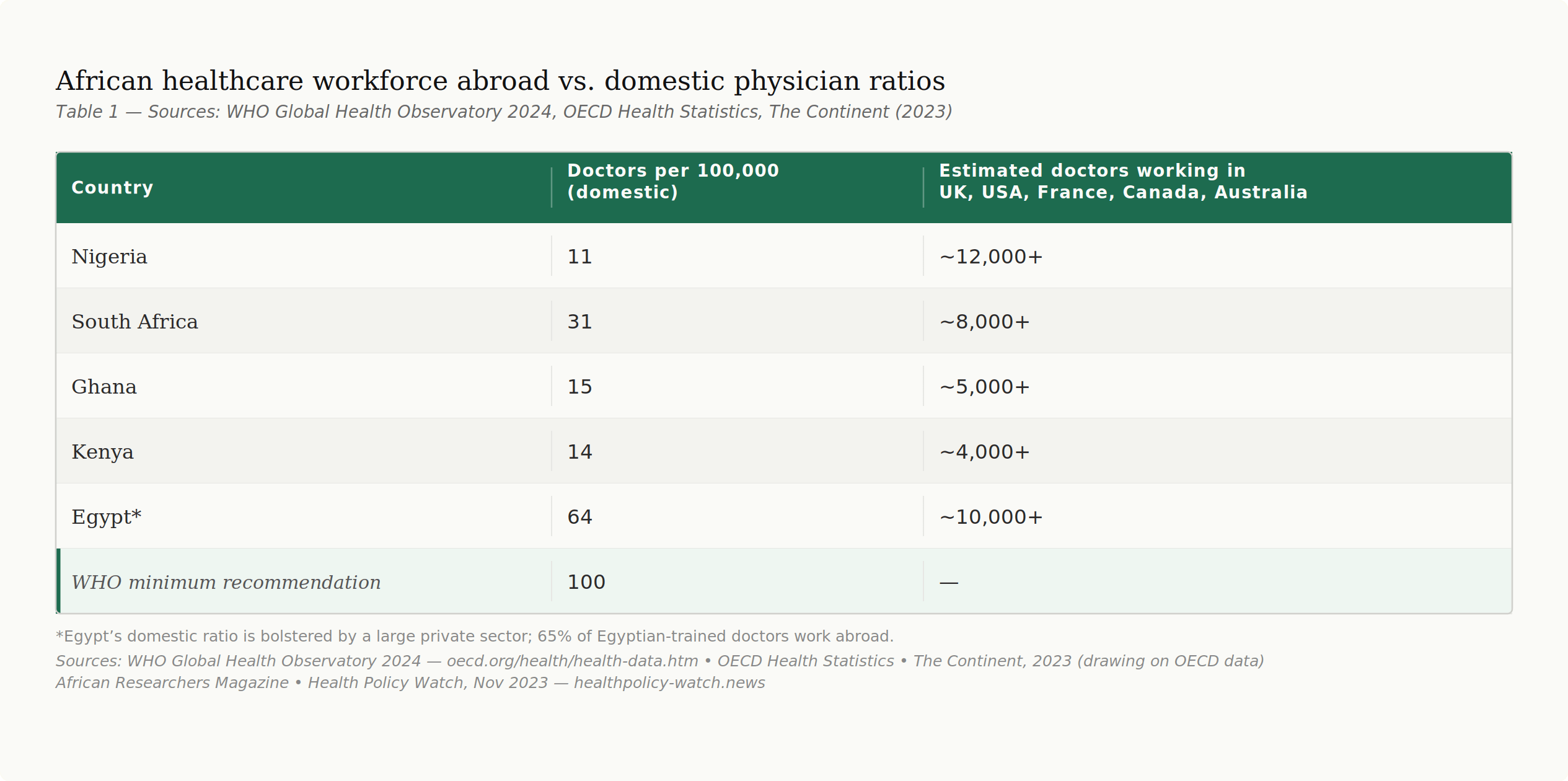
Now let’s get nerdy. I promise this pays off.
According to a 2023 data analysis by The Continent, drawing on the latest OECD figures, fifteen of the world’s wealthiest countries host over 55,000 African doctors who qualified before entering those countries. The United Kingdom leads as the top recipient, followed by the United States, France, Canada, Germany, and Ireland, in that order. The underlying OECD data shows that Egypt has lost the most doctors of any African country, followed by Nigeria, South Africa, Algeria, and Sudan. Africa, providing all of this talent, has 3% of the world’s health workforce despite representing 11% of the global population and bearing 24% of the global burden of disease, according to WHO estimates cited in peer-reviewed research.
The financial dimension of this is addressed as diversity, if at all. The United Nations Conference on Trade and Development has estimated that each migrating African professional represents a loss of $184,000 to the continent. When the cost of educating a single medical doctor is compounded over a working lifetime, each emigrating doctor costs their country of origin approximately $517,931 in lost returns on public investment. South Africa alone, with 600 of its medical graduates registered in New Zealand, has faced an estimated financial cost of $37 million from that one emigration corridor. And yet, in what ought to be the punchline of a very dark joke, Africa spends $4 billion a year on the salaries of 100,000 foreign experts. The continent is exporting its trained professionals and importing foreign replacements at significant cost to the public purse. We’re out here running a very expensive revolving door and calling it development.

THE TECH ARGUMENT, WHICH IS NEWER AND EQUALLY INTERESTING
Healthcare is the most visceral version of this story. Alongside education it’s also among the easiest ones to feel guilty about, which is probably why it gets the most attention. But the architecture of extraction runs through many sectors.
According to the PEW Research Centre, roughly 73% of H-1B workers whose applications were approved in the United States in fiscal year 2023 were born in India, with China accounting for 12%. The majority of Silicon Valley’s technical workforce is foreign-born. The companies building the infrastructure of the modern digital economy are dependent, in ways their marketing materials do not emphasise, on talent produced elsewhere.
Global technology companies trumpet the mission of global connectivity and remain substantially staffed by people from countries whose citizens struggle to get the visa required to visit the company’s headquarters (my personal favourite structural irony of the last decade). Stated plainly, there are systems in place to recruit doctors, nurses, engineers and developers through formal programmes and specialised visa pipelines. These skilled workers will be tasked to build technical infrastructure with their expertise because using them is simply more efficient. And the consequences of this extraction will be described as a drain.
THE DRAIN IS NOT A NATURAL DISASTER
“Brain drain” suggests a passive, regrettable process. It may be the kind of thing you might describe with a sympathetic shrug at a development conference before moving on to the next agenda item. The movement of skilled professionals from “developing” to “developed” countries is actively recruited, structurally incentivised, and in many cases bilaterally negotiated by governments.
The Kenya-UK Bilateral Agreement on healthcare workforce was signed in 2021. By April 2024, it was reported that 280 Kenyan nurses had migrated to the UK under it, with approximately 200 more awaiting placement. This is a policy. Not a drain. The UK government signed a document that said, in clear terms, we would like some of your nurses, and Kenya agreed, partly because it cannot absorb all of its graduates into a public sector that is itself chronically underfunded. Kenya currently has an average of 10- 14 medical doctors per 100,000 people. The OECD average sits above 21.

The push and pull factors are well documented. Healthcare workers across Africa earn between $200 and $500 monthly, while their counterparts in developed countries earn multiples of that. Nobody leaving is making an irrational choice. They are making the most rational one available to them, inside a system that was structured to make that choice rational for them and efficient for the countries receiving them. What is rarely asked, with any seriousness, is who structured the system and in whose interest.
WHAT THE HAEMORRHAGE ACTUALLY COSTS
I’m calling this a haemorrhage rather than a drain because a haemorrhage implies something your body cannot afford to lose at the rate it is losing it. The physician-to-population ratio across Africa sits at approximately 13 per 100,000. Africa has 3% of the world’s health workforce and 18% of its population, and approximately 23,000 qualified academics emigrate from the continent every year.
This is not a talent pipeline problem or a question of individual ambition outpacing national opportunity. It is a compounding structural deficit that widened over decades, accelerated by bilateral agreements that receiving countries drafted with their own labour shortages in mind, and legitimised by a development discourse that consistently frames collective loss as individual opportunity.
As I mentioned, my mother did not go abroad. She remained in South Africa, and continued nursing years after that recruitment opportunity. She is still sharp and still entirely too practical for most conversations. One Zulu man and his very particular views on geography kept at least one trained nurse on the continent. I am not entirely suggesting we start building health workforce retention strategies around patriarchy. But I am suggesting that a national system sent someone to recruit her, and that we should be precise about what that means and who absorbs the cost when the answer is yes.
Until I pick up the pen again,
NMN
Postscript
This series is my attempt to map the infrastructure of movement: what it costs, who it serves, and what we are not saying out loud about any of it. If this essay brought something up for you, tell me in the comments. If you know someone who needs to read it, send it. I may never write exactly what you suggest, but I have never seen a suggestion box commit a crime.
I’m glad this resonates. (Quick huddle: are we building a group of #daughtersofthepatriarchy?) Lol.
Real talk, happy it sticks. True witnessing the reaction towards groups of people who were recruited for their skills, now being treated as though they came to squatter in their own accord is so jarring.
There is so much to the conversation on global mobility … the individual financial gain with emigration, the personal and professional experience of being an immigrant, the cultural dynamics of global teaming, the economy of remittance. It’s such a complex topic with wide reach impacting those who leave, who stay and who have to interact with a new workforce.